

Schizophrenia is a psychological disorder that causes clinically significant level of disruptions in various aspects of an individual’s life; socially, occupationally, educationally, and in daily life. It can also impair a person’s ability to think effectively, regulate emotions, make decisions, and interact with people. Schizophrenia affects about 24 million people, or one in every 300 persons (0.32%) worldwide.[1] individuals with schizophrenia are often diagnosed between their late teens and early twenties, with women exhibiting symptoms later than men.
In this article, we will break down several common misconceptions surrounding schizophrenia.
Causes multiple personalities (DID):
Dissociative identity disorder (DID), often known as split personality disorder, is a disorder in which you have two or more distinct personas that influence your actions at different times, leading to gaps in memory. The formation of multiple identities is typically caused by trauma. [2]
The main difference between DID and schizophrenia is that DID involves distinct personality states, whereas hallucinations or psychosis has episodes. There is no set number of episodes an individual with schizophrenia may have, this is in no way related to having distinct personalities and identities.
Is inherently dangerous:
Schizophrenia, other psychotic disorders and personality disorders are most often associated with violence than with any other disorder. This is further reinforced by the way the media portrays these individuals.
Rather, people with schizophrenia are more prone to injure themselves than others. Not only that, but because of the influence of hallucinations and delusions on their thinking, individuals are more likely to engage in harmful behaviour such as suicide or violence when experiencing acute psychotic symptoms. However, one crucial component is that co-morbidity with substance abuse leads to a higher chance of aggressive behaviour. An individual with schizophrenia is fifteen times more likely to engage in dangerous activity if they abuse alcohol or illegal drugs. [3]
According to research, between 10% and 15% of individuals with schizophrenia behave violently, which means that between 85% and 90% do not. [4]
Is a result of a traumatic childhood:
Schizophrenia does not have a single known cause, but rather a combination of genetic and environmental factors that can contribute to its development.
Schizophrenia is estimated to be 60-80% hereditary. Research has shown a series of genetic abnormalities with origins called endophenotypes, which can be inherited. Gottesman and Shields (1966) conducted a twin study examining monozygotic and dizygotic twins. The twins were identified through blood tests and fingerprint analysis. Some parents were also interviewed and examined for any previous diagnoses of schizophrenia. The results of this study were backed by Fischer (1930) who showed that that the concordance rate in monozygotic twins is around 50% and 10-19% in dizygotic twins.
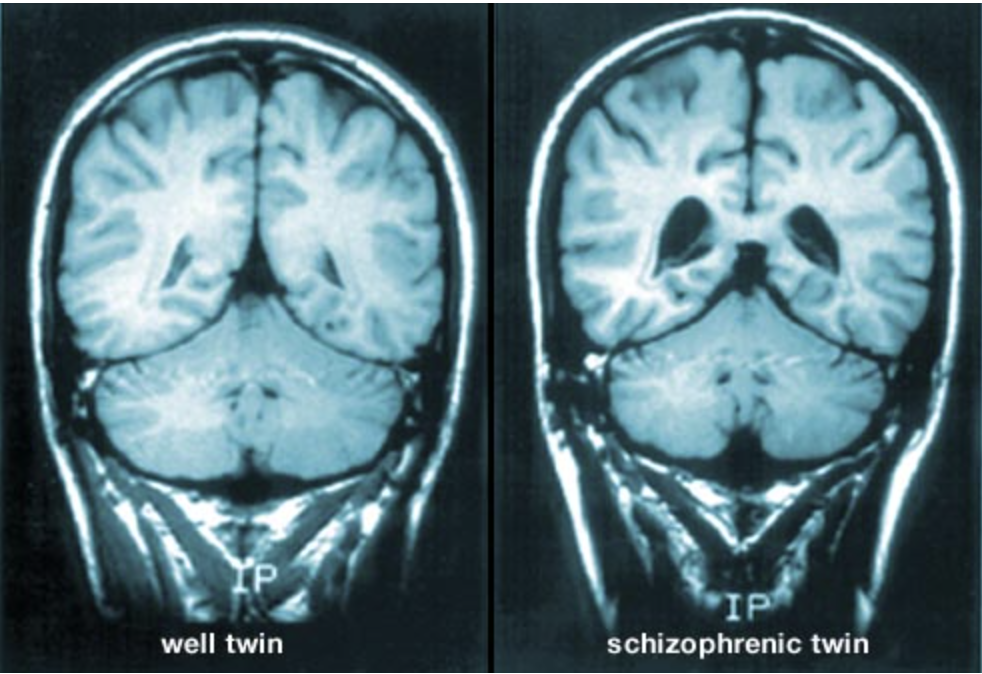
^the ventricles (dark spaces) are much larger in the schizophrenic brain. [5]
The biochemical explanation focuses on the dopamine hypothesis found by Lindstrom et al in 1999. This hypothesis states that the brains of individuals with schizophrenia have extra sensitive receptors to dopamine, which them disrupts the normal transmission of nerve impulses. Drugs such as cocaine and amphetamine increase dopamine levels and can cause hallucinations and delusions. PET scans use cameras to detect radioactive tracers. These tracers accumulate in areas of high activity which show that there is a large amount of dopamine in that area. High levels of activity equal positive symptoms and low levels of activity equal negative symptoms.
Difficult life circumstances, like trauma or neglect can often increase the risk of developing schizophrenia or make its symptoms more severe. It is important to distinguish between risk factors and causes. Childhood adversity is linked to the severity of symptoms in people who already have schizophrenia or are at risk.
Fun fact: Individuals born in certain seasons—like late winter or early spring—may have a higher chance of developing schizophrenia. Source: DSM-5-TR.
Is curable:
Schizophrenia is a lifelong disorder and is not curable, but it is treatable. With therapy, the symptoms can be managed.
Schizophrenia can often be treated using a combination of antipsychotic medication. First generation antipsychotic drugs block dopamine and serotonin receptors in the corticol and limbic areas of the brain. A test done via RCT and the double blind placebo trial found that 50% of patients taking antipsychotics showed significant improvement in 4-6 weeks, 30-40% showed partial improvements. However, first generation antipsychotic drugs have unpleasant side effects such as TB, EPS, drowsiness and weight gain. Second generation antipsychotic drugs are as effective as first generation rugs but are less likely to produce EPS and TB, however they do lead to weight gain and obesity. Third generation antipsychotics produce even fewer side effects which prevent patients from being deterred from taking the medication.
Healthcare professionals may consider electroconvulsive therapy (ECT) for adults with schizophrenia who may not respond to antipsychotic medication or those with catatonia. It is not meant to replace the medication but rather to work in conjunction with it. Electroconvulsive therapy (ECT) is a procedure done with general anaesthetic and this uses electrodes to pass a small current not lasting longer than a second to induce seizures which last upto a minute. Patients regain consciousness in around 15 minutes. The seizures itself are used as a treatment in aims to ‘restart’ the nervous system. The electrodes are applied to the non-dominant hemisphere of the brain to reduce memory loss.
Another option is long term psychotherapy which can help with tackling the secondary problems associated with schizophrenia, such as anxiety, depression or substance use issues. Cognitive Behavioural therapy can also be used as it focuses on improving the patient’s ability to cope with schizophrenia by identifying thoughts and behaviours and helping restructure them. It incorporates cognitive and behavioural approaches the patient can utilise outside of therapy.
Token economy is a treatment that focuses on operant conditioning. Paul and Lente examined 84 individuals split into 3 groups over 4.5 years. In the token economy, patients were rewarded with a token if they displayed appropriate behaviour such as self care or attending therapy sessions. These tokens could be exchanged for luxury items such as sweets or cigarettes. The findings of this study showed that 97% of the group could live independently. This highlights how therapeutic interventions such as utilising a token economy can help patients reintegrate back into society and lead a more stable lifestyle.
These misconceptions are further solidified through media portrayal. The media often portrays individuals with psychotic and personality disorders as crazy or dangerous, feeding negative perceptions and stigmatisation. Not only that, individuals with schizophrenia may actively engage with the discourse surrounding their diagnosis, influencing how they are perceived and treated by others, impacting their social interaction and self-esteem. Overall, the language used to characterise any mental disorder has the potential for change, influencing attitudes, viewpoints, and actions. It is important to utilise proper discourse and to raise awareness to break down stigmas surrounding all psychological disorders, increasing awareness.
REFERENCE:
- (2022, January 10). Schizophrenia. World Health Organization.
- DID vs. Schizophrenia: What’s the Difference? (2023, February 13). Healthline.
- Living With Schizophrenia. (2012). Schizophrenia and Dangerous Behaviour – Living With Schizophrenia. Living with Schizophrenia.
- Singh, J. P., Serper, M., Reinharth, J., & Fazel, S. (2011). Structured Assessment of Violence Risk in Schizophrenia and Other Psychiatric Disorders: A Systematic Review of the Validity, Reliability, and Item Content of 10 Available Instruments. Schizophrenia Bulletin, 37(5), 899–912.
- Psychology Wizard. (2005). Gottesman & Shields AO1 AO3. Psychology Wizard.